Ahsan Numan1,
Faisal Masud2,
Khadija Irfan Khawaja2,
Fehmeda Farrukh Khan2,
Abdul Basit Qureshi3,
Saira Burney2,
Kamran Ashraf4,
Nisar Ahmad4,
Muhammad Shahbaz Yousaf4,
Imtiaz Rabbani4,
Hafsa Zaneb4,
Habib Rehman4 ![]()
For correspondence:- Habib Rehman Email: habibrehman@uvas.edu.pk Tel:+24299212871
Received: 6 January 2016 Accepted: 5 September 2016 Published: 31 October 2016
Citation: Numan A, Masud F, Khawaja KI, Khan FF, Qureshi AB, Burney S, et al. Clinical and electrophysiological efficacy of leaf extract of Gingko biloba L (Ginkgoaceae) in subjects with diabetic sensorimotor polyneuropathy. Trop J Pharm Res 2016; 15(10):2137-2145 doi: 10.4314/tjpr.v15i10.12
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To investigate the health benefits of Gingko biloba L. leave extract EGb 761 in patients with diabetic sensorimotor polyneuropathy (DSP).
Method: In a randomized, double-blind, placebo trial, patients (n = 156) received Gingko biloba (120 mg/day) or placebo for 6 months. Efficacy of Gingko biloba extract EGb 761 was assessed on the reduction in the scores of “Short-Form McGill Pain Questionnaire” (SF-MPQ) and improvements in latency, amplitude and conduction velocity of four sensory (ulnar, median, peroneal and sural) and four motor (ulnar, median, peroneal and tibial) nerves.
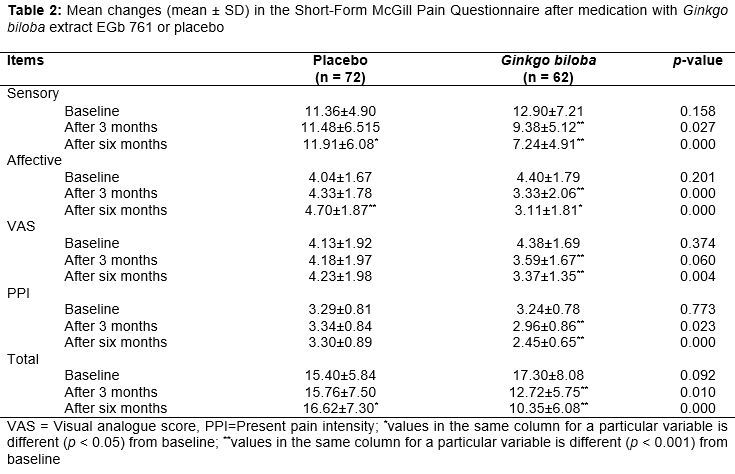
Results: Gingko biloba significantly improved the mean scores of sensory, affective, visual analogue score (VAS) and present pain intensity (PPI) of SF-MPQ on 3 and 6 month post-treatment. At the start of experiment in the Gingko biloba-treated group, scores for sensory, affective, VAS and PPI domains were 12.90 ± 7.21, 4.40 ± 1.79, 4.38 ± 1.69 and 3.24 ± 0.78 respectively. After 6-months treatment with Gingko biloba, scores for sensory, affective, VAS and PPI domains were reduced (p < 0.01) to 7.24 ± 4.91, 3.11 ± 1.81, 3.37 ± 1.35 and 2.45 ± 0.65 respectively. Contrarily, in the placebo-administered group, sensory domain was (p < 0.01) deteriorated after 6 month (4.70 ± 1.87) compared to the baseline (4.04 ± 1.67). Gingko biloba extract EGb 761 failed to influence the electrophysiological measures when compared with the placebo group. The common adverse effects observed with Gingko biloba were somnolence and dryness of mouth compared with the placebo-treated patients
Conclusion: Gingko biloba extract EGb 761 seems to be an effective and safe drug for reducing symptoms of DSP without any apparent effect on the electrophysiological attributes of sensorimotor nerves.
Introduction
Diabetes mellitus (DM) is known worldwide seen in many parts of the world including the developing countries [1]. In Pakistan, nearly 5 million people are affected with DM, and this number is expected to rise by 13.9 % in the year 2030 [1]. A complex form of neuropathy known as diabetic peripheral neuropathy (DSP) can result due to persistent high glycemic serum level. Diabetic polyneuropathy is a symmetrical, length-dependent sensorimotor polyneuropathy resulting from alterations in metabolic and microvascular factors due to chronic hyperglycaemia [2].
Generally, diabetic neuropathic syndromes have been divided into two major classes: symmetrical neuropathies and asymmetrical neuropathies [3]. Diabetic sensorimotor polyneuropathy (DSP), a distal and symmetrical form of neuropathy, is commonly encountered [4]. Persistent hyperglycemia triggers neuropathy by eliciting degenerative changes. These degenerative changes consist of demyelination, axonal atrophy, nerve fiber loss, and distorted repairing of nerve fibers. The DSP often interferes with sleep and results in significant pain characterized by ‘aching, burning, stabbing, and/or also include tingling sensations. [5].
Consistent efforts were made in the last decade to find effective treatment for DSP. Aldose reductase [6,7], tricyclic antidepressants, serotonin norepinephrine re-uptake inhibitor (SNRI), certain anticonvulsants and opioid analgesics are commonly being used to treat DSP, but often the efforts become limited because of variable efficacy or unacceptable side effects [8]. Ginkgo biloba leaves extract is used to ameliorate Alzheimer’s disease, depression, vertigo, hearing loss, short-term memory loss, lack of vigilance or attention and diabetes mellitus [9]. Success of Ginkgo biloba application is because by its main active ingredients flavonoids (flavone glycosides, quercetin) and terpenoids (ginkgolides and bilobalides). A previous study demonstrated the neuro-modulatory effects of Ginkgo biloba on cortical neurons and hippocampus in rats [10].
It has been found that Ginkgo biloba supplemented diets prevented early onset of DM and improved various electrophysiological indices of motor and sensory nerves in rats [11,12]. Quercetin has been shown to decrease thermal hyperanalgaesia and cold allodynia in diabetic rats [13]. Ginkgo biloba is reported to be effective in various functional characteristics and histological features of injured sciatic nerve in a rat model [14,15]. Oxidative stress leads to vascular, microvascular and specific tissue complications in diabetes, therefore oxidative stress modifiers play a pivotal role in therapy of DSP [16]. However, there is a dearth of knowledge about the potential use of Ginkgo biloba in attenuation of deteriorating effects of DSP in human. The present study aims to evaluate the potential use of leave extract of Ginkgo biloba extract EGb 761 in reducing the severity of pain and restoration of functional characteristics of peripheral nerves in patient of DSP.
Methods
The study was carried out from April to December, 2011 in men and women (aged > 18 years) visiting the Diabetic Management Centre, Services Institute of Medical Sciences (SIMS), Lahore, Pakistan. Diabetes mellitus type 2 (DMT2) the patients were diagnosed based on plasma glucose levels of ≥ 126 and ≥ 200 mg/dl on fasting and two-hour postprandial, respectively. Patients with following conditions were not included in the study: Pregnant, breastfeeding subjects, renal dysfunction (serum creatinine level of > 1.3 mg/dl), hepatic dysfunction, myocardial infarction, myocardial ischemia, cerebrovascular disease or past history of any cardiovascular, psychiatric disorders, diabetic neuropathy (e.g., phantom limb pain from amputation) or cutaneous problems at the site of neuropathy. Exclusion criteria also included the use of tricyclic antidepressants, neuroleptics, centrally acting sympathomimetics, MAO inhibitors, acetaminophen, or opioids or any other un-identified therapy from non-professional medical practitioners.
Patients who were taking chronic analgesics, antidepressants, capsaicin topical cream, were considered for screening only after a four-week washout period. Aspirin (for prophylaxis of myocardial infarction and transient ischemic attacks), acetaminophen (4 g/day) and stable doses of serotonin-re-uptake inhibitors were allowed if prescribed by registered medical personals. The study was approved by Institutional Research Board of Services Institute of Medical Sciences, Lahore and recruited participants were provided informed consent. The confirmed patients of DMT2 were assessed for the presence of clinical DSP using Michigan Neuropathy Screening Instrument [17]. Participants showing score of ≥ 3 were designated as diabetic individuals with clinical DSP. The MNSI includes two separate assessments: a 15-item self-administered questionnaire (called history) and a lower extremity examination (physical assessment) that includes inspection and assessment of ankle reflexes and vibratory sensation [17,18]. The current study was in accordance with the guidelines of Good Clinical Practice and Declaration of Helsinki [19]. Before the start of the study, the Institutional Ethical Review Board, Services Institute of Medical Sciences, Lahore approved the protocol of the study (Notification no. IRB/28/C-SIMS dated 05-11-2009). The enrolled participants were informed about the experimental procedure before allowing them to enter in the study.
Experimental design
This was a randomized, double-blind, placebo-controlled study in DMT2 patients with clinical DSP. Patients were randomly assigned to Ginkgo biloba extract EGb 761 (120 mg/day) or placebo. Randomization was computer generated. A sample size of 132 patients underwent clinical trial to evaluate and compare the efficacy and safety of the Ginkgo biloba and the placebo. To assure blinding, the medication was prescribed in 2 bottles, each containing capsules having 120 mg Ginkgo biloba or placebo. The patients were prescribed to take one capsule daily after breakfast. The blind was maintained till completion of study and data evaluation. The patients were asked to visit the Outdoor Clinic, Department of Neurology, SIMS, Lahore after 3 and 6 months of treatment. The patients were also advised that they may either visit the clinic or may seek medical guidance on telephone if needed weekly. However, the outcome measures were investigated 3 and 6 months post treatment.
Outcome measures
The efficacy of the Ginkgo biloba extract EGb 761 was assessed based on reduction in the pain scores using “Short-Form McGill Pain Questionnaire” (SF-MPQ) and improvement in the electrophysiological attributes of selected motor and sensory nerves. During the course of the study, the patients were also asked to register any adverse effect on diary to assess the drug safety. The SF-MPQ is a well-validated multidimensional pain questionnaire [20,21] and was filled at the start of treatment and subsequently 3 and 6 months post intervention.
The electrophysiological parameters (latency, amplitude and conduction velocity) of four motor nerves (ulnar, median, tibial, peroneal) and four sensory nerves (ulnar, median, sural, peroneal) were studied with the aid of an electro-myograph (Nihon Kohden Toshiba, Japan) as described earlier [7]. Mean NCS measures were compared at baseline and endpoint.
Safety analysis
Safety was evaluated at every visit by obtaining record of concomitant medications, body weight, heart rate and blood pressure. Blood samples were collected at first visit and then at 6 month post-intervention for the determination of hematology, glycosylated hemoglobin (HbA1c), glutamate pyruvate transaminase, creatinine and lipid profile. Adverse effects observed during the clinical trial were recorded.
Statistical analysis
Data are expressed as mean ± SD and percentage. All tests were performed using Statistical Package for Social Science (SPSS for Windows version 12, SPSS Inc., Chicago, IL). The level of significance was set at p < 0.05. Demographic information was analyzed using the independent t-test for continuous variables and Chi-square test for categorical variables. Independent student t test was performed to determine between group variations (placebo vs. treated groups). One-sample paired t-test was employed to compare the means of scores and electrophysiological measures from baseline to 3 and 6 months separately.
Results
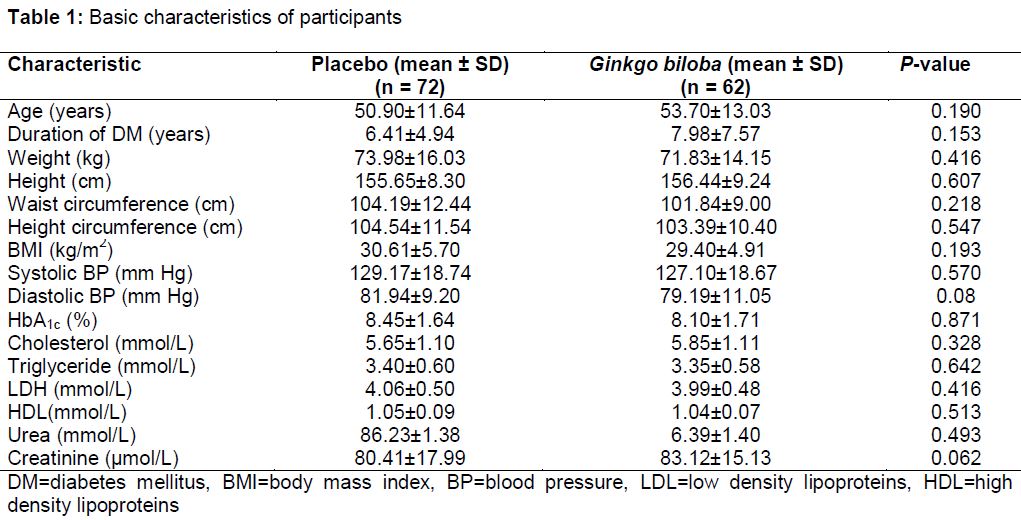
Of the 156 patients screened, 4 were ineligible because of violation of selection criteria at entry and withdrawal of consent. A total of 152 subjects were randomly distributed in two groups with 76 patients in each group. A total of 134 (88 %) of the 152 recruited subjects completed the six months study without any notable protocol violation. In the placebo group, 4 patients were withdrawn due to absence during follow-up leading to 94.73 % response rate. For the Ginkgo biloba-treated group, 14 (5.26 %) subjects could not complete the study either due to absence during follow-up or failure to return or serious deviation from protocol. As shown in , baseline demographic characteristics and serum metabolites of the Gingko biloba-treated and the placebo groups were nearly balanced (p > 0.05).
Efficacy of Ginkgo biloba extract EGb 761
Analysis of SF-MPQ revealed that baseline values of sensory, affective, VAS, PPI and total (sensory plus affective) scores were similar (p > 0.05) in both groups (). The patients treated with Ginko biloba showed significant improvement in the sensory, affective, VAS, PPI and total scores compared with the placebo group on both time scales. In the Ginkgo biloba group, there was a progressive decrease in the affective, VAS, PPI and total scores from baseline to 3 months and 6 months post-treatment. In the placebo group, the mean scores were higher for sensory (p < 0.05), affective (p < 0.001), and total domains (p < 0.05) respectively, after 6 months compared with the baseline level ().
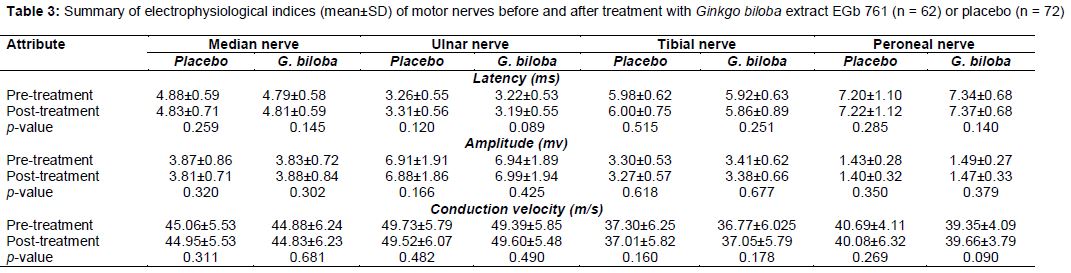
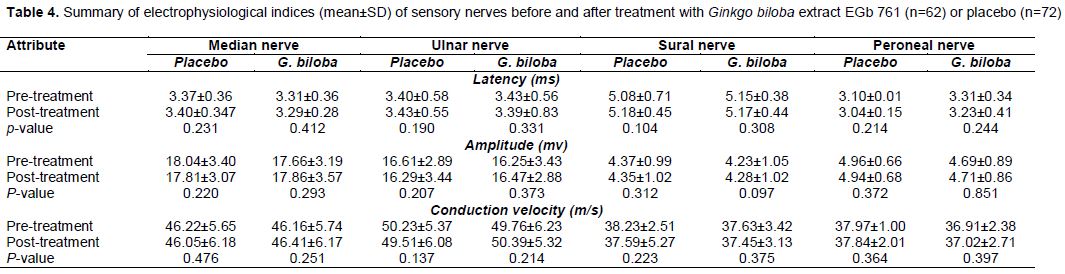
Latency, amplitude and conduction velocity of four motor nerves were similar (p > 0.05) in both groups before and after treatment (). There was no significant improvement in the electrophysiological parameters of motor nerves in the placebo group over 6 months treatment period when compared with the baseline. Similar outcomes were observed for the Ginkgo biloba-treated group when electrophysiological measures of baseline phase were compared with the post-treatment time. However, conduction velocity of motor peroneal nerve tended to be higher (p = 0.09) at the end of treatment compared with the baseline. The Ginkgo biloba also marginally improved the latency of motor ulnar nerve after treatment (p = 0.089). Similarly, Ginkgo biloba medication did not influence the latency, amplitude and conduction velocity of sensory nerves when compared with the placebo group (). There was also no difference in the electrophysiological attributes from baseline to endpoint in both study groups.
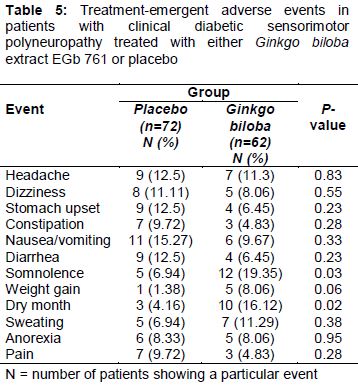
Adverse events in the placebo and the Ginkgo biloba-treated groups are summarized in . The severity of dry mouth and somnolence were significantly higher (p < 0.05) in Ginkgo biloba-treated group compared to the placebo group. Generally, the untoward effects were mild or moderate, except dry mouth that was more frequently (p < 0.05) noticed in the Ginkgo biloba-treated group compared with the placebo-treated group ().
Discussion
Painful neuropathy is quite common in the patients suffering from diabetes and may have adverse effects on quality of life [22]. Management of diabetic pain is a vital element in the care of diabetic patients with painful clinical polyneuropathy. In the present randomized, double-blind, 6-month placebo trial, we demonstrated that Ginkgo biloba significantly improved the subjective outcome measures in the patients of DSP without any apparent effects on electrophysiological attributes of sensorimotor nerves. Daily dose of 120 mg of Ginkgo biloba was chosen based on information from prior clinical studies [23-26] suggesting a dose-response relationship up to 240 mg [26]. Ginkgo biloba has been reported to protect various types of neurons in the central nervous system including cerebellum [27], cerebral cortex [28], basal ganglia [29], hippocampus [30] and retina [31] in various disorders like ischemia and oxidative stress.
A body of evidence shows that sustained hyperglycemia is closely related to oxidative and nitrosative stress that can initiate development of diabetic complications like DSP [32]. Oxidative stress has been recognized as one of the fundamental mechanisms involved in development of DSP [33]. In the current experiment, changes in the subjective pain scores in SF-MPQ were used for the evaluation Ginkgo biloba. During the study period, difference between the subjective symptom scores of the Ginkgo biloba-treated group and the placebo group increased over the time. Ginkgo biloba improved subjective symptom scores compared with the placebo group.
In the Ginkgo biloba-treated group, reduction in the sensory (-5.66), affective (-1.29), PPI (-0.79), VAS (-1.01) and total scores (-6.95) was recorded when compared with the baseline score. On the contrary, differences in the scores from the baseline of all the domains were increased in the placebo group (055, 0.66, 0.01, 0.1 and 1.22 for sensory, affective, PPI, VAS and total scores, respectively).
It has been found that Ginkgo biloba contains many pharmacologically active components like flavone glycosides (kaempferol, isorhamnetin, quercetin) and terpen lactones like ginkgolides A, B and C and bilobalide [34]. Quercetin is a powerful antioxidant and has been reported to decrease thermal hyperanalgaesia and cold allodynia in diabetic rats [13]. Ginkgolide A has been found to suppress the production of pro-inflammatory cytokines to protect against cytokine-induced neuronal toxicity [35]. Moreover, multiple antioxidant components of Ginkgo biloba are believed to be responsible for most of its protective effects in neurons like scavenging of superoxide anions, peroxyl radicals, nitric oxide and inhibition of xanthine oxidase activity [36-39]. Therefore, the efficacy of Ginkgo biloba extract EGb 761 in managing the diabetic neuropathic pain in the patients might be due to its analgesic, antioxidant and anti-inflammatory potentials.
Electrophysiological measures were included to assess the potential role of Ginkgo biloba for restoring the functionality of peripheral sensorimotor nerves involved in the pathogenicity of DSP. Values of electrophysiological indices of the sensorimotor nerves did not vary between the Ginkgo biloba-treated and the placebo-treated groups. Pain is transmitted through small or unmyelinated fibers, but routine NCS is used to investigate large myelinated fibers. Therefore, the absence of any significant improvement in the electrophysiological measures between pre- and post-therapy phases is reasonable [40].
Our data also establishes that 6-month treatment with Ginkgo biloba extract EGb 761 seems to be safe and effective in the subjects having painful DSP as no notable treatment-related adverse event was noted despite more patients in the Ginkgo biloba-treated group experienced somnolence.
Conclusion
Ginkgo biloba extract EGb 761 has demonstrated a significant improvement in the subjective symptom scores of the patients of DSP without influencing any damaging or otherwise adversely affecting nerve function. Although there was no sufficient objective evidence of improvement of electrophysiological measures in the Ginkgo biloba-group, however, there was evidence of subjective improvement in patient pain which is widely considered as an effective measure of treatment in clinical practice. Therefore, it is safe to conclude that improvement in pain combined with partial functional improvement in few motor nerves is encouraging and, therefore, Ginkgo biloba extract EGb 761 may be developed as a drug for managing clinical DSP in patients.
Declarations
Acknowledgement
References
Archives


News Updates